SKIP A STEP & SAVE MONEY…do I need to see my GP or Podiatrist for a foot complaint?
Podiatry
A podiatrist is an Allied health professional in foot care. Podiatrists help people in the care of their lower limbs including the foot and ankle and may also be involved in supporting older people to reduce their risk of falling.
They can treat conditions such as toe fungus, ingrown toenails, corns, calluses, bunions, infections and foot injuries. Podiatrists can perform ingrown toenail surgery using a local anaesthetic.

Where do podiatrists practice?
Podiatrists mainly work in private practices but also work in a range of health settings including hospitals, aged care, sports clinics and research and policy organisations.
When should I see a podiatrist?
There are a wide range of reasons to see a podiatrist but some typical foot conditions include heel pain, bunions, ingrown toenails, tinea, plantar warts, corns and calluses. Some typical examples of why someone might see a podiatrist are:
- Patient with diabetes and peripheral vascular disease, or neuropathy
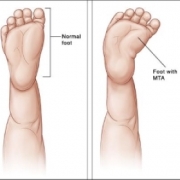
- Clinical diagnosis or history of foot or lower limb deformity
- Clinical diagnosis of falls
- Arthritis
- Soft tissue and muscular pathologies
- Circulatory diseases.
What services do podiatrists provide?
Podiatrists provide a wide range of services from the treatment of calluses to the treatment of bone and joint disorders. For conditions such as recurring sprains and chronic pain, podiatrists may prescribe foot orthoses.
The podiatrist’s scope of practice includes areas such as paediatrics, diabetes, sports injuries, structural problems, treatment of the elderly as well as general foot care.
Podiatrists with additional qualifications and registration may also perform foot surgery.
How are podiatrists qualified?
In order to practice in Australia, a podiatrist must complete the following:
- A Bachelor of Podiatry
- Australian Health Practitioner Regulation Agency (AHPRA)
- Continuing professional development.
Skip a step and make a direct booking with one of our qualified podiatrists today on 5223 1531